Pesquisa
US Quiz of the Month – May 2022
A 64-year-old female was referred for general surgery department for common bile duct (CBD) abnormal dilatation. Her previous medical history included dyslipidemia and depression and she was currently medicated with propranolol, lorazepam and sertraline. Previous surgeries included cholecystectomy, appendectomy and thyroidectomy. Magnetic resonance cholangiopancreatography (MRCP) revealed CBD dilation with a maximal diameter of 14 mm and mild dilation of intra-hepatic bile ducts. Although there were no intraluminal lesions, the dilation appeared to end abruptly at the junction with main pancreatic duct (Fig. 1).

Therefore, she undergone endoscopic ultrasound (EUS) that confirmed CBD dilation and hyperechogenic contents were apparent at its distal portion suggestive of biliary sludge. Prompt endoscopic retrograde cholangiopancreatography (ERCP) was performed, but no calculi were identified at cholangiogram or after Fogarty balloon exploration. There were no immediate adverse events.
At the following day, the patient complained of abdominal pain and performed an abdominal computerized tomography (CT) where moderate ascites was noted. Laboratory studies revealed leukocytosis and elevated C-reactive protein. Diagnostic paracentesis was consistent with biliary peritonitis and she started intravenous antibiotic therapy with ceftriaxone and metronidazole. Considering a possible biliary perforation, ERCP was repeated. There was no evidence of contrast leakage. Nevertheless, considering biliary ascites, a fully-covered self-expandable metal stent was placed (Fig. 2).
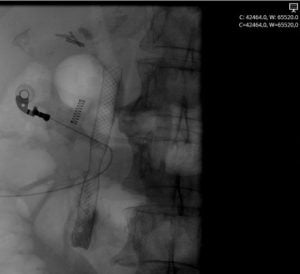
Figure 2. ERCP fluoroscopy: biliary fully-covered self-expandable metal stent placed.
She maintained antibiotic therapy for 14 days with clinical and biochemical improvement and undergone repeat abdominal CT which revealed three abdominal fluid collections: one with 14.9×6.9×7.8 cm at retroperitoneal location, one with 6.6×3.4 cm adjacent to gastric posterior wall and one with 8.6×4.2 cm at the Pouch of Douglas (Fig. 3).

Figure 3. Axial abdominal CT: three abdominal fluid collections.
After 2 weeks, she undergone reevaluation EUS where the largest collection had reduced in size, with 57×35 mm, but still extending from liver to spleen along left subphrenical space and it was multiseptated with honeycomb appearance (Fig. 4).

Figure 4. Linear EUS: multiseptated collection with honeycomb appearance.
WHAT WOULD BE THE NEXT STEP?
DISCUSSION
Considering the patient’s favorable evolution and absence of evidence of complications during radiological work-up, a decision to follow a conservative approach and maintain close surveillance with short-term reevaluation was taken.
Biliary peritonitis is usually a manifestation of bile duct perforation that has rarely been reported after ERCP and is usually associated with surgically damaged liver tissue, liver metastasis or abscesses (1-3). Early diagnosis and prompt treatment is essential in the management of post-ERCP perforation and CT has proven to be the most useful imaging method. However, preoperative diagnosis of spontaneous bile duct rupture is challenging despite advances in the diagnostic procedure. When the leak cannot be visualized macroscopically, intraoperative cholangiography following cholecystectomy is considered to be useful (4). The treatment can be conservative or surgical, although in recent times, endoscopic treatment with clips has been more frequently employed (5).
Although in our case there was no evidence of overt perforation from radiological work-up and surgery was not attempted considering favorable evolution with conservative management, biliary peritonitis is likely to have been caused by bile duct rupture following ERCP. Notably, this case demonstrates that conservative management may be an option in this situation.
REFERENCES
-
Karačić A, Batur P, Štritof D, et al. A Novel Cause of Biliary Peritonitis after Endoscopic Retrograde Cholangiopancreatography: Case Report and Literature Review. Case Rep Gastrointest Med 2021;2021:3814080.
-
Khan Z, Darr U, Nawras M, et al. Pneumoperitoneum after Endoscopic Retrograde Cholangiopancreatography due to Rupture of Intrahepatic Bile Ducts and Glisson’s Capsule in Hepatic Metastasis: A Case Report and Review of Literature. Case Rep Gastroenterol. 2017;11(3):603-9.
-
Assimakopoulos SF, Thomopoulos KC, Giali S, et al. A rare etiology of post-endoscopic retrograde cholangiopancreatography pneumoperitoneum. World J Gastroenterol. 2008;14(18):2917-9.
-
Fukui T, Chochi T, Maeda T, et al. Biliary Peritonitis Caused by Spontaneous Bile Duct Rupture in the Left Triangular Ligament of the Liver after Endoscopic Sphincterotomy for Choledocholithiasis. Case Rep Gastroenterol. 2021;15(1):53-61.
-
Jin YJ, Jeong S, Kim JH, et al. Clinical course and proposed treatment strategy for ERCP-related duodenal perforation: a multicenter analysis. Endoscopy. 2013;45(10):806-12.
AUTHORS
Emanuel Dias1, Raquel Gonçalves1, Renato Medas1, Pedro Moutinho-Ribeiro1, Guilherme Macedo1.
- Gastroenterology Department, Centro Hospitalar Universitário de São João, Porto, Portugal.