Pesquisa
US Quiz of the Month – Novembro 2024
Case Report
We present the case of a 73-year-old female patient evaluated in consultation for long-standing dyspeptic symptoms. Her medical history included osteoporosis medicated with calcium, vitamin D and denosumab every 6 months. The patient underwent an upper endoscopy that described a 10 to 15 mm subepithelial lesion (SEL) on the anterior wall of the proximal gastric body, with hard consistency when touched with biopsy forceps (Figure 1). No other relevant findings were documented. Gastric and SEL biopsies showed no morphological abnormalities.

Figure 1. Upper endoscopy: 10-15 mm subepithelial lesion located in the anterior wall of the proximal gastric body (1A – front view; 1B and 1C – retrofllexed view).
Subsequently, the patient underwent a computed tomography (CT) scan, which revealed normal gastric wall thickness without expansive lesions, perigastric findings or any notable changes. The CT scan also revealed a normal sized homogenous liver with residual scattered microcalcifications.
The patient was then submitted to endoscopic ultrasound (EUS), that demonstrated a slight 10 mm bulge on the anterior wall of the gastric body, corresponding to an oval structure with well-defined borders, slightly heterogeneous but predominantly hyperechoic, with an acoustic shadow. It seemed to be either associated with the gastric serosa or possibly the liver (Figure 2).
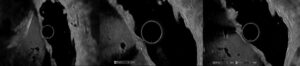
Figure 2. EUS: oval structure measuring 5.3×4.4 mm with well-defined limits, hyperechogenic and producing an acoustic shadow, appearing to be dependent on the stomach serosa or at the periphery of the liver.
The CT scan images were reviewed and an hyperdense image in the topography of the gastric SEL was identified (Figure 3).
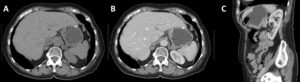
Figure 3. CT scan: stomach distended with water with normal thickness wall, and an hyperdense image near the gastric wall (2A – axial view; 2B – axial view contrast-enhanced; 2C – sagittal view).
What is the most likely diagnosis?
Discussion
The imaging studies obtained, as well as the review of the CT scan images, are highly suggestive that the LSE represents a peripheral hepatic calcification causing compression of the anterior wall of the gastric body. Hepatic calcifications can be seen in a wide variety of disorders, including infections (such as bacterial, parasitic, and fungal infections), biliary, vascular diseases (such as hepatic artery aneurysm and intrahepatic portal vein thrombosis), granulomatous diseases, neoplasms (both primary and secondary), or traumatic lesions. Worldwide, the most common causes are granulomatous diseases, neoplastic lesions, and hydatidosis.
In the case presented, the calcification was not associated with a focal hepatic lesion, such as cystic, target, hypo/hypervascular lesions, or lesions with progressive enhancement. The most common causes of isolated calcifications in the liver are infections, particularly those resulting in granuloma formation, and traumatic lesions. Tuberculosis and histoplasmosis are the most common infections associated with granuloma formation, and the presence of calcified granulomas in the lungs and spleen aids in the diagnosis of granulomatous diseases.
CT is the most sensitive imaging technique for detecting and evaluating hepatic calcifications, and the widespread use of this examination will likely lead to an increase in the incidental diagnosis of these lesions. It is important to note that morphologic appearances alone do not allow for a specific diagnosis; the association of other imaging findings, clinical presentation, and laboratory tests may indicate the correct diagnosis or help narrow the differential diagnosis.
References
- Mamone G, Di Piazza A, Gentile G, et al. Imaging of calcified hepatic lesions: spectrum of diseases. Abdom Radiol (NY). 2021 Jan 16;46(6):2540-2555. doi:10.1007/s00261-020-02924-6
- Agnello F, Rabiolo L, Midiri F, et al. Focal hepatic intrinsically hyperattenuating lesions at unenhanced CT: Not always calcifications. Clin Imaging. 2021 Aug 27;80:304-314. doi:10.1016/j.clinimag.2021.08.020
- Patnana M, Menias CO, Pickhardt PJ, et al. Liver Calcifications and Calcified Liver Masses: Pattern Recognition Approach on CT. AJR Am J Roentgenol. 2018 Apr 18;211(1):76-86. doi:10.2214/AJR.18.19704
- Paley MR, Ros PR. Hepatic calcification. Radiol Clin North Am. 1998 March;36(2):391-398. doi:10.1016/s0033-8389(05)70030-0
Authors
Margarida Cristiano1, Nuno Almeida1,2, Margarida Ferreira1, Pedro Figueiredo1,2
- Gastroenterology Department, Unidade Local de Saúde de Coimbra, Coimbra, Portugal
- Faculty of Medicine, University of Coimbra, Coimbra, Portugal